|
home
definition
evaluation
of the airway
difficult airway algorithm
face mask
tracheal
intubation
laryngeal mask

|
Optimal position for endotracheal intubation
Successful laryngoscopy
involves the distortion of the normal anatomic planes of the
supralaryngeal airway to produce a line of direct visualization from the
operator's eye to the larynx: this requires alignment of the oral,
pharyngeal, and laryngeal axes.
A number of criteria must be
met if this is to occur:
 the
oral aperture has to be adequate to allow visualization (and
instrumentation), the
oral aperture has to be adequate to allow visualization (and
instrumentation),
the
tongue must be small (relative to the oral cavity and mandibular space)
and pliable
enough to allow its distortion,
the
mandibular space (the area between the mentum and the hyoid bone) must be
able
to accommodate the tongue as it is displaced by the laryngoscope.
|
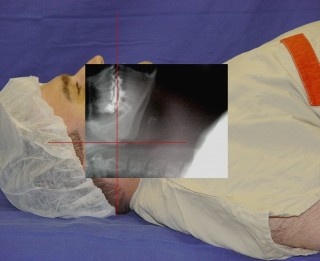
an optimal “sniff”
or Magill position

Failure to maintain
this position during laryngoscopy is one
of the most common
reasons for a
poor-grade laryngoscopic view. |
This position, which
entails a slight flexion of the neck on the thorax (35°) and severe
extension of the head on the neck (an 80–85° angle between the
sagittal axis of head at level of nose, and the long axis of neck) at
the atlanto-occipital joint, accomplishes the best possible alignment
of the oral, pharyngeal, and laryngeal axes |
|

|
identify the cricothyroid
membrane |
|
The “sniff” or Magill
position opens the airway, moves the epiglottis out of the visual
line, and maximally reduces airway resistance.
The Magill position can be
accomplished in the clinical setting by placing a "small pillow"
under the head, while the shoulders remain flat on the patient
surface.
|
 |
top
 |
neutral position |
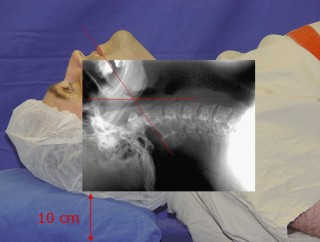 |
“sniff” or Magill position
|
|

With the morbidly obese
patient, a "small pillow" may not provide a position adequate
for laryngoscopy.
|

A wedge-shaped lift is
used to move the mass of the morbidly obese patient's chest away from
the area of laryngoscopy and to improve the compliance of the thoracic
cavity. |
top
|
www.airwaycam.com

BURP maneuver
|
 |
|
If, during the laryngoscopy, a
satisfactory laryngeal view is not achieved the
backward-upward-rightward pressure (BURP) maneuver may aid in
improving the view.
In this maneuver, a second operator
displaces the larynx:
(a)
backward against the cervical vertebrae,
(b)
superiorly as possible and
(c)
slightly laterally to the right, using external pressure over the
cricoid cartilage.
 |
The BURP maneuver has been shown to
improve the laryngeal view, decreasing the rate of difficult
intubation. |
|
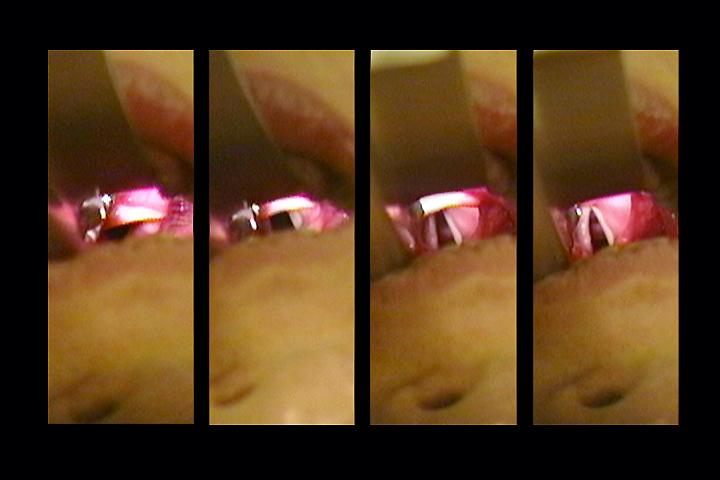
Cormack-Lehane classification system
|
Cormack-Lehane grade:
I = most of the glottis is visible;
II = the posterior commissure is visible;
III = no part of the glottis can be seen
except the epiglottis;
IV = not even the epiglottis can be seen.
|
top
|
